
+ 51 How do different esters work together?
Most of us know by now how esters work and their importance in our cycles. I would like to share my opinion on how different esters work with each other to coalesce into a single stream. Different esters release free testosterone at different rates. This is common knowledge; the question is what happens to that testosterone once released from the ester? It is my intention to illustrate this question in the simplest and most straightforward way possible.
Disclaimer:
I am in no way a medical professional, PhD or pharmaceutical representative. I am an engineer and math is second nature. That being said the following post is my opinion based off of pharmacokinetic equations and theories. I have charted any and all graphs, illustrations and tables using Excel.
Abstract:
This paper is about how different esters combine to create a homogenous stream of testosterone primarily using Sustanon 250 as a basis. I will first illustrate how a basic Testosterone enanthate ester releases a daily amount of free testosterone into the bloodstream. I will then illustrate how this affects our plasma levels and leads into a taper. This will demonstrate how different esters can affect our PCT and the importance of timing to maintain and or keep our gains. Finally I hope to generate questions that will lead to more in-depth considerations on the subject.
How esters work
By now I think most of us understand how esters work. Each ester has a specific half-life that cleaves off testosterone into the bloodstream, acetate and propionate being amongst the shortest of the esters. Consequently decanoate, undecanoate and cypionate being the longer esters take more time to release free test into the bloodstream. Starting off with testosterone enanthate we know that the half-life is 8 to 10 days. This means that approximately every 8 to 10 days the original dosage is cut in half (Half Life Math). Now testosterone enanthate has a test base of 70%. This means that for every 100 milligrams of testosterone enanthate there is approximately 70 mg of testosterone. It is therefore surmised that every day 70% of the daily dosage released is freed to attach to receptors. So imagine if you will a large stream flowing through a ravine. Now imagine a tributary connecting to that stream that flows into a larger body of water. The mainstream in this case is the testosterone flowing to the receptors in our bodies and the tributary is the ester releasing free testosterone to flow into the mainstream. See illustration 1.
So for illustrative purposes let’s take a single shot of 100 mg of testosterone enanthate. Knowing what we know about the half-life of this ester at day two we would have 91.7 mg in our body. Now the difference between the 100 mg and 91.7 mg would be 8.3 mg. 70% of that 8.3 mg would be 5.81 mg of free testosterone. (At this point I would like to make it clear that we are dealing with just milligrams for the entire body, the actual plasma level is represented using the nomenclature nanograms per deca-leader or ng/dl). At day three we would have 84.09 mg of enanthate in our system cleaving off the difference between 91.7 and 84.09 multiplied by 70% equaling 5.33 mg of free testosterone and so on and so forth. So you can see that the free testosterone is 70% of the difference between day one, day two, day three and so on. See table 1.
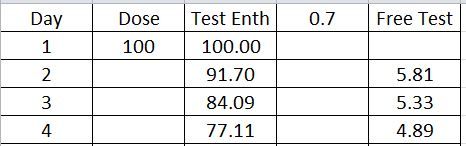
Table 1
If we were to use the table above as an example starting with a 100 mg shot then we would see that over the course of 71 days it would release small amounts of testosterone into the mainstream daily until it reached zero. Graphically it would look like illustration 2.
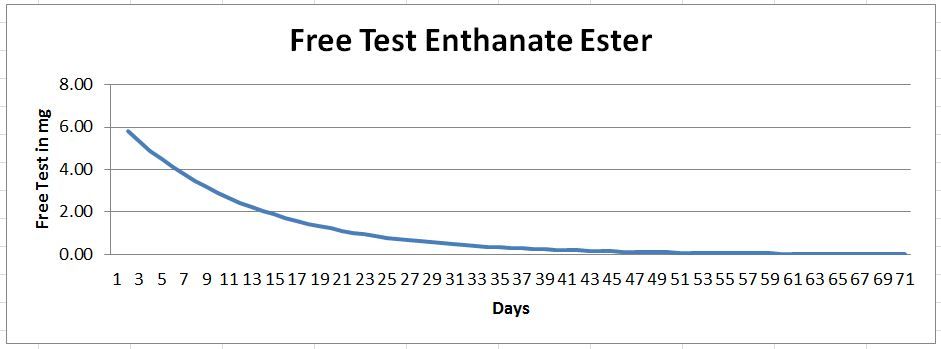
Illustration 2
It is easy to see at this point how the last injection or known amount of testosterone tapers off naturally. This is sort of analogous to a steep cliff wherein one could easily fall down and crash. This is what is meant by a post cycle crash. It is the point where natural production of testosterone cannot ramp up to the previous levels introduced through extraneous injections. This leads into a proper taper at the end of the cycle mitigating the painful loss of gains due to post cycle crashes. This is relevant to our PCT regiments in that if one could calculate the amount of short ester testosterone necessary to gradually reduce or lessen the slope of the curve, we could give our bodies more time to rebound back into a homeostatic state. I will address this point shortly.
Test is test
The heading says it all. Using the theory of a homogeneous stream of testosterone we can expound on the principle that esters work individually to contribute to that very stream. What I’m saying here is that it doesn’t matter what testosterone blend or ester we use, each blend or ester releases testosterone daily or hourly even at its own rate, but it all goes to the same stream. We will use the classic Sustanon 250 as an example. Starting with Testosterone Propionate at 83% with the half-life of two days all the way to Testosterone Decoanate at 63% with a half-life of 15 days, we will see how each ester individually contributes to the mainstream. See table 2.

Using the table above and the previous analogy of a large stream running through a ravine with several different tributaries connecting to it we would get a graphical representation like illustration 3.
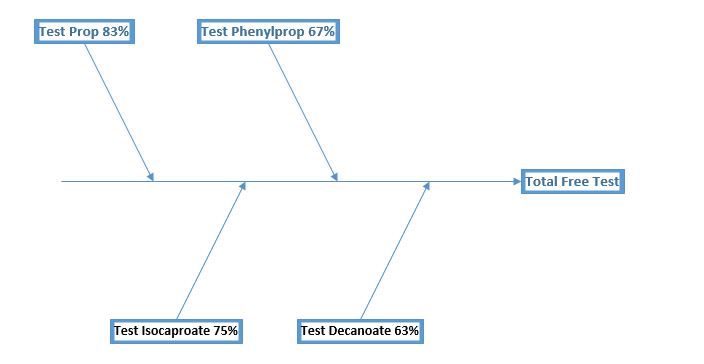
Illustration 3
The mainstream of test is now free to bind to other receptors. What’s important to note here is that each ester releases its own specific amount on an hourly basis until it has diminished itself to zero. So starting with Testosterone Propionate at 30 mg would take approximately 24 days to reach zero and Testosterone Phenylpropionate at 60 mg would take 44 days to reach zero followed by Testosterone Isocaproate at 60 mg would take 87 days to reach zero and finally Testosterone Decanoate at 100 mg would take a whopping 140 days to reach zero. See illustration 4.
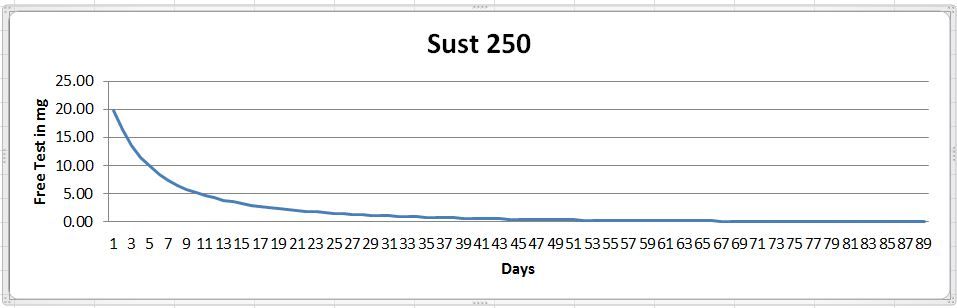
Illustration 4 (In this graph at 90 days the amount is actually .05 mg of test, it actually takes 140 days to reach zero)
Notice how steep the slope is with only one shot this explains why intervals are spaced so closely together when running a Sustanon cycle. However, this begs the question; how much test needs to be in our system to shut down natural production? This would be a huge factor in when we start PCT.
Putting it all together
So knowing that esters release testosterone at an individual rate let’s see what a simple Testosterone enanthate cycle would look like at roughly 1000 a week for 10 weeks with a two-week Propionate taper. See illustration 5
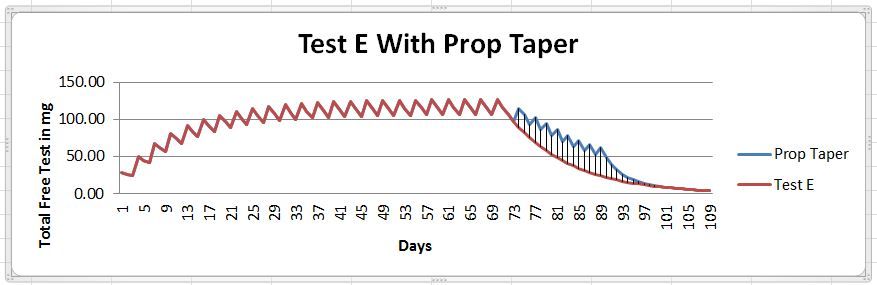
Illustration 5
Keep in mind these graphs represent the actual testosterone in the blood and not the ester. I make this point so as not to get confused with my previous graphs on other papers.
In this illustration I’m showing a Test E cycle of 12 weeks. However, I have stopped the enanthate ester at 10 weeks. This is where it gets interesting if I were to immediately on the last day of the 10th week inject propionate to start my taper, I would see a noticeable spike above the 150 range. This is not really beneficial to us and in fact is extra shots and money. It is better in this case to start the propionate taper five days after the last enanthate shot. By using the propionate to taper we can see how much we can lessen the slope after cessation of a simple cycle which gives our bodies ample time for PCT to kick in.
I know this is way more in depth then most people on here want to get and you do not need to be able to do the math to understand these simple principles, however, by understanding how esters work together you may be able to build smarter and more efficient cycles and that's what it's all about. Right? Thank you for reading.
Other posts I have written that may help you understand the science behind this paper:
Half Life Math
Maximizing Cycles
C.H.
- Bookmark
- 51
- 0
I have read this a few times now. I am going to give it a thumbs down, for several reasons. Not calling anyone out, its not about Karma, just showing a different point of view, ideally to give a balanced and critically [critical thinking, rather than being critical of] thought out review which might make people think a little deeper on these really interesting subjects, I hope that makes sense Happy to change that if what i am saying/thinking is wrong/incorrect.
Reference: Comparative pharmacokinetics of testosterone esters, Hermann M. Behre and Eberhard Nieschlag
Keep in mind these graphs represent the actual testosterone in the blood and not the ester. - well 30mgs in the blood represents an approx 42 mg shot of testosterone given intravenously (~30/7x100=42)
Sure would we even survive that? So there is an error in there somewhere.
Then the taper itself. It is confusing, because it is showing individual esters on the graph, whereas it should actually be showing the combined ester, to display accurately what is happening within the blood plasma. There would be a spike off the test level and a subsequent return to the test base (although that base might be slightly* elevated). So, this graph is flawed iin the sense that it should show the individual contribution of a prop dose independent of the E (as is with the E displayed) and then a 3rd combined line needs to be plotted showing the combined action in nmol/l. The graph is misleading at best and doesnt addressed the combination and rest of a prop taper.
Hopefully this gives food for thought/continued discussion and not the usual naysaying with the world is still being flat and all that!!!!!!!!!!!!!!!
I think you're reading way too much into what the OP is trying to say.
This is a Steroids 101 discussion to help someone to visualize and be mindful of half lives and how combining different esters "work" in our body. You're like a theologian poo pooing a children's bible story version of adam and eve because it ignores the theological allegory and symbolism.
The use of Sust was as an example of an ester blend only; to illustrate how different esters and ratios combine to feed the "stream". Free Test is understood as test that has been cleaved from the ester.
dosage, mg's, pin schedules, the reality of susts unstable nature and why, true blood plasma levels, etc. are advanced concepts that fall outside of the intent of this post.
Perhaps you could post a more comprehensive, advanced version as a companion piece to this one
Everything goes right back to the OP's opening paragraph. He made his mission statement, and in my opinion accomplished just that in the simplest and most straightforward way possible.
Well you might be right, maybe I have looked into it too much, but if you are right about what I am like then you are poo poo'ing my poo poo'ing.....?! No homo!
Look this well written article is a step beyond steroids 101 and worthy of discussion - I would argue that steroids 101 would serve better if viewed in the plasma cycle, makes sense if talking about sides tests etc for the purposes of educating us all here n eroids (general ed ya know, relevant to actual usage/experiences?). Anyway, it is good to look deeper in general and any aspect of the OP's topic is really interesting..
The question was... "what happens to that testosterone once released from the ester" I am highlighting that this wasn't actually answered. There was no discussion or graphs for/for the post de-esterification phase (excretion/absorption to blood etc.)
The abstract says the paper is about how different esters combine to create a homogeneous stream of testosterone - But this is just not true. Different esters, eg those within sust, or prop with test E actually disrupt the stream. This doesnt mean we shouldn't do a prop taper etc. BUT, if we are going to highlight a prop taper, you have got to look at pin schedule/plasma levels - steroids 101 as discussed every day here.
I really dont think that the different esters "disrupt the stream"
you get a unique curve when you combine short and long esters.. a fast spike and a long taper compared to a mid ester like plain ol test E or C
Its still gonna be released on a steady "curve" in graphing language. no lumps or bumps in the curve.
here's one in the archives that I was hoping to rehash... but Tread is no longer a member... I dont believe.
https://www.eroids.com/forum/general/general-talk/test-prop-and-counting...
Well, they do disrupt it as I see it. Yes you do get a fast spike (a disruption), much more pronounced than single ester, and you get a drop off to the longer ester base or just below it (another disruption)... thats a big difference, unless we are talking about 2 different things when we discuss stream, but i dont think we are??? Maybe I an't understanding you, and if not accept my apologies.
So OP said homogeneous stream, however the delivery/the stream is anything but uniform. It changes the pharmacokinetics of the unesterified test within the body in a negative way. Remember the curves are usually displaying a mean, particularly computer generated images. Have a look at the following images.
Fig 11.4 shows the best fitting line which = the curve whereas the the closed circles show the mean +/-SEM from data measured in real plasma,. In an single individual those closed dots will vary even more. This proves there is no even homogeneous stream even with a single ester of Test E. Note the up / down levels of the actual plasma mean+/- SEM, the stream is in a constant state of flux. Therefore multidose single esters in vivo have this state of flux all the way up and down the peaks and toughs, similar to what we might see on a financial traders screen, if you can picture it?
Fig 11.7 shows the 3 (best fitting) lines of tes e, prop and a combination, for a single dose. Not the huge spike for the combo, returning to the test E level. This is single dose only but shows both a different movement of the drug in the system (test is not test, a stream is not a stream, esters matter etc.)
Fig 11.8 Again shows a (best fitting) simulated curve plotted on the upper graph, but this time for a multi dose combination of prop and test e. You can see the way the pharmacokinetic profile has changed the peaks and troughs, mean less stability within plasma, and more sides.
Now what is missing here, is the actual taper. So using your steroid calculator but for mg of unesterified compound, see the blue image showing the test e cycle of 250 e3.5d 1-10, then 12-13 of a prop 100mgEOD taper. The gap between peak and trough (sides) is pretty big and there is no uniform stream, and an even steeper drop-off/cliff at the end of the prop cycle, again back to the test e base level (which may or may not be desirable depending on the individual). In an actual individual rather than sim, the peaks and troughs would vary even more.
The reality is that the combo changes the stream/pharmacokinetics of the drug in vivo, but yes we can absolutely manipulate if we choose, as the OP already said.

What do you make of it with this info in mind?? Curious to get your thoughts....
Top images from Behre's book already referenced and blue image from http://steroidcalc.com
image: https://preview.ibb.co/gfWWSv/a1a1a1_NEW1.jpg
I dont see this as a disruption, just the normal release of a short ester. If you get sides from the peaks and troughs of short esters than simply avoid them, or pin every day... or even multiple times a day.
The graph you have plotted at the with test e followed by a test prop taper is just kinda sloppy. To much time between the end of test E and the start of prop. If a guy wanted to he could keep things far more stable by adjusting the dose of prop as the test E tapers off and pin more frequently.
Personally, I'm ok with fluctuations.... I feel great after pinning some TNE, and feel fine the days after
I see what you're saying but the compound effect results in a change in pharmacokinetics and not a normal release. The graph is as close to the OPs suggestion as I could figure on your site - yes very sloppy as you say and highlights the disruption in a similar - reality can be worse - timing, pin schedule, tapering a taper can all become important in reality if we seek a smooth return with less sides (obvious or otherwise).
But as I say, and in agreement with you, we can adjust and tailor all of these things to suit our individual needs/prefs.
Again I think his point was to demonstrate how we can use different esters to our advantage, e.g. you can use a car to drive from point a to b. He wasn't trying to discuss how to drive nor how to navigate.
One, unrelated question I had asked the OP a long time ago, was if there was a way to find out what dose would be an approximate net 0 or net loss.
I.e., If my natural test levels were 900 and I started taking exogenous test which suppresses my own production, what dosage would I need to break even? For example, if I took 200mg test cyp a week and it shut me down, my levels could be 600 to 800 visa ve the exogenous test; which would be a net loss of 100 - 300 from my natural level of 900.
Also un-graphed is on day one, my natural levels + the cleaved "free test" = X with the natural levels in decline as the exogenous test levels rise.
That's a brilliant question. I suppose the + of shutting down natural production is the relative stability of the exog test levels. I would imagine the subjective factors like bodyfat %, inj site chosen etc. will make it a variable dose. You wont find the answer in a book though, unless willing to look at averages and test from there.
Its an interesting point though, and I think that it is the reason you hear of some TRT guys saying they feel absolutely, even though they have low-normal levels of test - 3-400 etc. - They just have not hit the right dose to come close to what was normal/should be normal for them.
Trial and error I guess!
yep, they say estro is 100x as suppressive as test, so your conversion to e2 must be the largest factor for when you quit making LH and FSH...
It's also the basis for the low test dose cycles. Im planning at the moment based on that to see if I can keep the E2 in check as much as possible. Id say 75% of problems we encounter are Estro related
RustyhookerTo each his own. Cant see the forest thru the trees.
Smh....
There's been more learned on this site by users, blood and pro bodybuilders than any desk reference can ever serve. Real Drs still push test gel or bimonthly injects. Proof in the pudding is its utter failure. Those cliffs do in fact fall steeply. Esters cleave off, hormone used and excreted. Or we'd simply use 1 pin and be jacked. Suspensions half life in real world use is excellent in describing the importance of pinning by the hour on half life. A book can try to reinvent the wheel but its not feasable in real use
If you can't see the forest from the trees Rusty then you need to open up your eyes!
Those cliffs do in fact fall steeply - Which ones? the real ones as I have said, or the illustration showing "free test" release/disposal rates?! You are echoing my point.
Suspension - Yes exactly!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! Therefore in real world terms, the plasma levels are where the rubber meets the road for product efficacy, but for PCT/different esters you need to dig deeper.
A book can try to reinvent the wheel but its not feasable in real use - Yes exactly!!!!!!!!!!!!!! - The book I referenced is of clinical research primarily and discusses bloods, supraphysiological doses etc etc etc. So you can consider it a guidebook whether a TRT user, pro bodybuilder or whatever you like.
Rusty, you seem to think you are arguing against my points, but you have actually agreed and reinforced them. Thank you sir.
RustyhookerEasy enough to write a thick saucey forum of your own citing all the pharmacokkawhatevers. You really should do it. And see how it flies.
Folks here wont read past the intro. They only wanted and asked for the basics which the op filled completely.
You wanna get into jargon bookie Wookieepedia? Smartest dude in this site is Area. He is the Dr of pharmawhatevers. You see more than 5 replies onhis posts? Noone wants book magic.
Roids been around since 1935. And SURPRISE, but theres been no new roids in over 3 decades. Yes the pros like arnold ran parabolan etc. Nothing is new. And the constant is bodybuilding 101. The cycles havent changed. The gear and taboo hasnt changed.
Just write your fancy reports that lose the basics. Like last report. Folks fell out because noone gives a crap about being a chemist. They want basic knowledge and to grow.
Why don't you two step back a bit. There's no reason this needs to be contentious.
RustyhookerTheres no anger. Id like to read his report. Its much easier than shredding a great forum. Might teach new angles too.
I've read your rebuttal, I'm going to have to give it a thumbs down.
I got what the author meant about the esters combining, I think most of us reading did. While the use of sust was a poor example ( sust is kinda obsolete) he got his pint across.
The author may use the term "free testosterone" in a context that is not synonymous with its use in blood work, we understand that he means test that is not locked up in the depot of the testosterone ester.
Illustration 2 is referring to the initial steep crash of supraphysiological levels and the extended duration of the sub physiological levels that would in layman's terms, be high enough to interfere with PCT but low enough to have you feel crappy.
the illustration with Test E and a Test P taper is just fine. It accounts for the change in pin schedule from E4D to E2D and a drop in mg per week of exogenous test. plug those esters and mg into http://steroidcalc.com/ looks correct for a taper.
While the med papers and research out there throws around half lifes, terminal half lives, mean residence time etc... we've seen the studies that show blood serum levels relative to dose.
For test E, the half life of the serum test level is about 4.5 days.to 5 days
If a guy has a test level of 1000 on the day 1 after a pin, at day 7 he will be about 450
these ratios stay about the same regardless of dose.
I didnt really neg you, I like the discussion and we all benefit from digging deeper into these matters.
Hey CBBurr, spot on fella. Discussion is only a good thing. Even educated/informed arguments are a positive. Respect.
On your points:
No its not. Its flawed on many levels, but primarily because the prop addition will cause a more sever set of spikes at EOD and drops only to at or just above the enth curve. I did plug the numbers into the calc and it clearly shows this for ester release rate, but if you read the book section on combined esters, it shows the same thing for plasma levels.
I plugged in 15 weeks, but showing 25 weeks... 500mg test e3.5 weeks 1 thru 10, and then 100 prop EOD weeks 12 thru 15. Day 103 mgs are at 83, day 123 mg's are at .01 (which is essentially zero).
Switch off the prop in the calc, and you also get a far smoother, but longer transition to zero, but also .01 at day 123.
So... in summary this illustration is wrong and in reality the taper at EOD leads to worse peaks (= sides) and a steeper slope/dropoff, but shorter duration to zero. However, zero is not relevant, because the body will actually rebound before that point. (but when?! - which is a question the OP considers, in reverse).
the half life of the serum test level is about 4.5 days.to 5 days This is absolutely correct. serum, or plasma half life is ~4.5 days+/-.
Serum levels matter, hence the EOD versus ED points I make. MRT matters because you can calculate 5x MRT to give an idea of when you should hit zero, but in reality you can when designing PCT roll back from
that point because you do not need to hit absolute zero for your body to have rebounded.
Here is my point... If we are going to discuss release time into the body, the release rates into the blood and into watery form where they are de-esterified as well as the total elimination time from the body, then we need to discuss also; plasma lifecycle, and the duration for which the compound in the body is physiologically effective (how many of those extra 60 days actually matter?? I don't know the answer to that but it will make an interesting read up. Semantics aside, that's where the rubber meets the road and the implication of the whole picture for PCT is important.
I've seen this before and read it but could not understand why I didn't give it a thumbs up! Forgive my senility and forgetfulness brother Cry_Havoc! Well, here you go my friend +2 for some very insightful information! Thank you kindly I'm also adding this to my favorites as an occasional refresher course and an occasional bump!
This is amazing knowledge. Thank you
Great read. Love technical and mathematical information on this topic.
Bumping because it's awesome reading
Thanks brother, this was good information.
Bump for Sunday reading!
I'm glad to see that all the esters have put aside their differences and are working together in a spirit of brotherhood and muscle building. ;-)
RustyhookerBump for learning
I appreciate it rusty! Guess there's not much interest this dynamic concept! Lol
RustyhookerAnother forum folks are arguing the importance of sust with ed pins because the short prop esters. 60 mg ÷ 7 days......doesn't make sence to me. I still like the front load method then work the esters.
Listen!........ if you really want to debunk broscience and try something really radical, try Sustanon ED.............. dont laugh bro you know i dont talk out my ass.
No need to stack anything with it.......... try it! and let your mind be blown!
Ive tried things not of this galaxy.... if it didnt hold credence i would never let it out from the deep recesses of my mind and share with anyone.
from viking.
yes i agree with you on the front load, gains wise ed pinning is best, also keeps bloods stable.
Are you quoting viking or is this from your experience?
Those are my words bro............ he has pasted that post in here.
If rusty is aiming his comment regarding frontloading towards my comments my answer would be this...........
Blast/cruise guys never need to frontload anything ever.
Standard cycling .. a prop kicker could be used but is not imperative if a normal 16wk sustanon cycle is in place because after the 4th week ALL the other longer esters have fully booted up so the ride is not all about prop and phenyl...... what gives a long sustanon run the major kick is the NEBIDO (Decanoate).... same difference in plasma build up as using Deca instead of NPP...... hope this helps.
Cry... you understand my methods so you know where i am coming from.
Absolutely I agree with your methods and do know where you're coming from. I think I was trying to discern whether flash was under the impression that rusty was trying to debunk the method of daily injections by bringing in the logic from another board. Not eroids. The fact of doing daily injections with sust has little to do with stabile levels, I mean how do you qualify stabile blood levels at that high dose? You are injecting esters that are 16 days so even at every 4 days your levels are going to be more than stabile and the differences between stability at every day and every four days would be negligible in my opinion. That being said I still think the closer your shot intervals the better the results! So it makes sense to inject four esters if your at a competition level. In fact, what if we wrote an intermediate cycle for a member at 125 mg daily. That would be 875 a week but would prove how strongly effective Vike's method would be.
I think the magic in Vike's every day injection is the quantity and how the synergy between the esters working together release test in the blood stream. That is 1750 mg a week. That's a lot more than a simple beginner cycle!
Front loading only serves one purpose. To get your levels up to the steady state dose as fast as possible. This is the level at which what is released is equal to or greater than what is injected. It takes a while to build up to 500 a week being released so doubling up the first few injections is helpful. If you are starting a cycle from scratch and have no base in your system this makes sense. If you are on trt or are cruising than it makes little sense since you already have a base compound running through your system. At this point the only thing you need to do is up the dose.
Sorry Vike I meant to just agree with you and then went off on a tangent aimed toward a general audience! Lol!
not at all bro, im trying to get a definitive answer myself, its all learning, just opening a discussion, it good hearing opinions from good folk like you guys, i meant no disrespect or anything to rusty, me and him are bros all good, debates are what we learn from, id like to hear more about others experience!!!! cheers
No offense taken bro. I did not perceive you as taking any position at all. I just did not understand what was being asked exactly.
RustyhookerWhen I run a big sus cycle I'll try the ed pins. It'll fit easier into a stack for sure.
RustyhookerNo sir. Wasn't at any comments you've made. Was talking to the normal daily guy going with a cycle of 500 mg sust per week. They get all juicy because the prop in there. But at 500 mg the prop is just 60 per week whereas a basic prop kicker is 100 eod. Just trying to get guys to read cryhavok posts and really work the esters.
yeah yeah bro... i was working with you not against you in any way....... more info for Makwa to be honest
I dont want new guys running ED sust to be honest, they need to learn esters really even before using sust ever, so they know whats happening when they hit the rollercoaster lol
RustyhookerIt's a bit of a different ride for sure. It gets odd at times when there's so much good info but it sits stagnant.
Ahh! starting to make some sense now. What I was thinking of doing for a sust run was pinning 1mg sust MWF and pinning 50mg prop on the other days for the kicker for the first 4 wks.
Glad that cleared it up a little bro....... using the prop the way you mention would have you mega unstable and if you ran it for numerous weeks that way you would be water bloated real bad........ with the ED sust run if you the carbohydrates under strict control (re-jigging throughout cycle) you should stay lovely and dry!..... in the past (mid 80s) i actually prepped for a show purely running sust because its all we had, diet was red hot strict and got down to around 7% BF which was adequate back then to be competitive but as the years pass the standards changed and we had to go down the super ripped route but still as big as we could get to keep the mass hungry crowds happy lol....... i feel lucky in a way that from the early 80s upto last year when i was last on a stage i have ridden both the aesthetic shape train and also had to plunge into the mass monster train, so yeah i got to taste both principles and had to totally change tactics to suit...... sorry for wandering i just had to jump my mind back to Sustanon days to explain how it responded with ED use
Viking, is it safe to say that the more stable your levels are at the less bloat you get?
I've been trying to keep an eye on the whole cause / effect of bloat and want to try every strategy to keep it to a minimum.
Answer would be yes to the stability aspect but the water control is down to the end user keeping a tight control on carbohydrate intake........... we cannot just say " ok this cycle i wil use X amount of carbs throughout!... what you must do is constantly monitor the grammage to basically to control subQ water from blinding cuts etc... we cannot go zero or ultra low carbs because we still want/need the muscle bellies themselves to be fully gorged to give to ultra swole appearence.
See this is why i constantly preach diet,diet,diet, if folks spent as much time researching how carbs/protein work and how minute changes in grammage can alter the physique they wouldnt need to feeling ill all the time running T3/T4 ECA stacks,high dose Clenbuterol and all the other fkn shit that is lethal... and what fucks me off/saddens me is this madness is just for "street use" not competition purposes.
Good sound knowledge about Nutrition and Training principles with the minimum amount of steroids is all that is needed to create the Beach body,chick pulling physique that most guys are looking for..... this is why i keep spitting out the term "Roid Junkie" because thats all most of these folks are, massive use of HGH, slin and a mega steroid array slapped on top with some thyroid manipulating sprinkles just for good measure!... its fkn madness and it makes me fkn laugh and cry at the same time because they are no better than fkn crack or heroin addicts and it makes a sham about the purity of what real Bodybuilding is all about.
Sorry for the essay bro... i just got on a roll there lmfaooooo its early here and im just winding myself up to go kill shoulders so that just got me in the mood to do some fkn damage
What I have noticed in my comp prep right now is just how much a small change in the amount of carbs affects my overall appearance and energy levels. I am sub 5% BF now and just a bump up in carbs of only 40g will fill out my muscle bellies and give me a surge in energy. I will also be about 1.5 lbs heavier the next morning from the added glycogen/water storage in my muscles and more vascular on top of that. I think what it boils down to is the body is much more insulin sensitive with lower BF. I won't notice much from a 40g change in carbs when my BF is higher. My next plan is to see how much of a change in carbs I need to elicit those effects with a higher BF. I think this directly ties into the post I made earlier that your BF should be as low as possible before cycling to take advantage of the increased insulin sensitivity.
Shit!.... my 6 teaspoon coffee just went cold as i wrote that............ what i sacrifice for eroids tut fkn tut ;/
Thank you for this one. ^^^
Saved my ass again with your knowledge bomb. Thanks
A lot of discussion lately about tapers and compound esters. So bump!
RustyhookerThoroughly enjoy your papers. Made me rethink my last sust/eq cycles taper to 5 weeks of shorts. Get the long hormones out of the equation so I'm not trying to reboot while basically still on cycle.
Is this something you plan on doing or have you done it Rusty? Would like to know how its going. I taper most all of my cycles now with great results!
RustyhookerNormally I taper 3 weeks. Last summer was big eq cycle with sust so tapered for 5 weeks. Simple mast p and tren a. No test and had no issues. The test took that long to cut out.